Basics
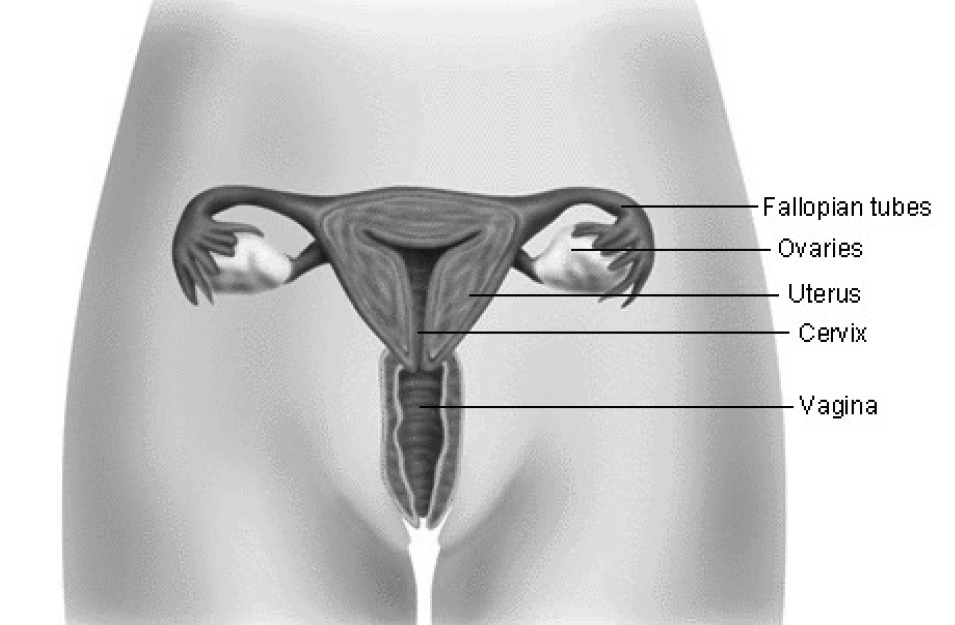
Cervical cancer begins when cells of the cervix undergo abnormal changes and begin to multiply. The cervix is the lower end of the uterus (womb) and opens to the vagina.
Cervical cancer is second only to breast cancer as the leading cause of cancer deaths in women worldwide. It can occur in women of any age who have reached puberty. Most cases (85% to 90%) involve the skin-like cells that cover the outside of the cervix. These cancers are called squamous cell carcinomas. Human papilloma virus (HPV), a virus that causes genital warts, is the primary cause in more than 90% of cervical squamous cell carcinomas.
The remaining 10% to 15% of cervical cancers develop in the glands that provide a mucus-like lubricant to the vagina. These tumors are called adenocarcinomas. In a few cases, a combination type of cancerous growth called adenosquamous carcinoma can occur.
With early detection, especially with Pap smears, nearly every case of cervical cancer can be prevented or cured.
Full-blown cervical cancer, medically known as invasive cervical cancer, usually takes years to develop. It typically starts out as dysplasia, a precancerous condition characterized by abnormal changes in cells.
The cellular changes cannot be seen by the naked eye and produce no symptoms. Fortunately, pelvic examinations and Pap tests (also known as Pap smears) can detect most precancerous conditions so that women can be treated before cancer develops. If left untreated, 10% to 20% of severe dysplasias will turn cancerous.
Cervical cancer can progress to penetrate deeply into the cervix. It can also spread to other areas in the pelvis such as the bladder or rectum, and beyond to other organs.
Causes
Cervical cancer occurs when cells in the cervix become abnormal and multiply out of control. These changes are often caused by human
Scientists do not know all of the reasons cervical cells turn cancerous. However, they do know that some viruses are strongly associated with the development of cervical cancer. Infection with HPV in particular can increase a woman’s chance of developing cervical problems that can lead to cancer. HPV, a virus that causes genital warts, can damage the cervical cells and lead to unregulated growth of abnormal cells.
There are many different types of HPV. Some HPV types are more likely to cause cervical cancer than others. These more harmful types are called cancer causing (oncogenic) HPV.
Symptoms
Cervical cancer often has no symptoms. This is especially true in the early stages of disease, when the cancer is most treatable. Therefore, it is extremely important for women to have routine Pap tests to detect early, precancerous cellular changes.
The American Cancer Society recommends that all women have a yearly Pap test starting at age 18 or at the age they become sexually active. Some clinicians think that if the results are normal for 3 years in a row, Pap tests need to be performed only every 2 to 3 years. Older women should continue to have Pap tests because a large percentage of deaths from cervical cancer occur in women aged 65 and older.
When symptoms do occur with cervical cancer, they include abnormal vaginal bleeding and pelvic pain.
Spotting between periods or bleeding after sex may occur with cervical cancer, but these symptoms may also be signs of other diseases or infections. Abnormally heavy bleeding during menstrual periods or bleeding after menopause could suggest cervical cancer. Unusual vaginal discharge is another possible symptom. In advanced-stage cervical cancer, pelvic pain, problems urinating, and swelling in the legs may occur as the tumor grows and presses on the blood and lymph vessels of the pelvis.
Because diseases other than cervical cancer can cause any of these symptoms, women experiencing them should consult a physician.
Early Signs and Symptoms of Cervical Cancer
- Bleeding or spotting between periods
- Bleeding after sexual intercourse
- Abnormal vaginal bleeding, especially irregular heavy bleeding
- Bleeding after menopause
- Unexplained vaginal discharge, particularly when it is thick or foul-smelling
- Pelvic (lower abdominal) pain
- Pressure on bladder or rectum
- Unexplained bladder irritation
If you are experiencing signs or symptoms of this issue, or have questions, you can schedule an appointment with us at our Baldwin Park office in Orlando, FL.
Risk Factors
Human papillomavirus (HPV) is the biggest risk factor for cervical cancer. HPV is a sexually transmitted disease (STD). Women often do not realize they are infected with HPV.
Infection with certain types of HPV, the virus that causes genital warts, greatly increases the likelihood of cervical cancer. Not all types of HPV lead to cervical cancer, and not every woman who has cervical cancer is infected with HPV. Studies performed by the United States government indicate that 6 million American women are infected with HPV but that only 15,000 women in the country are diagnosed with cervical cancer yearly.
Women who started having sex at a young age (before age 18) or who have had multiple sexual partners are at increased risk for contracting HPV, a risk factor for cervical cancer.
Having sex at an early age and having multiple sex partners are risk factors for any STD, including HPV. The sexual history of a woman’s partner is also important. A woman is at increased risk if her sexual partner has had multiple partners, is infected with HPV, or has had a partner with cervical cancer.
Women who smoke are at increased risk for cervical cancer.
Women who smoke are at least twice as likely as women who don’t smoke to get cervical cancer. Tobacco smoke contains chemicals that harm many tissues in the body. Even nonsmokers who are around cigarette smoke on a regular basis can have a higher risk of developing cervical cancer.
Women with weakened immune systems are at increased risk for cervical cancer. They also have a worse prognosis than other cancer patients if they develop the disease.
When the immune system is weakened, it becomes less able to find and destroy abnormal cells in the body, including cancer cells. Women who are taking drugs that suppress the immune system, such as women who have received an organ transplant, are at increased risk for cervical cancer. Women who are infected with HIV, the virus that causes AIDS, are also more likely to develop cervical cancer.
Women whose mothers took the drug diethylstilbestrol (DES) during pregnancy are at increased risk for a rare form of cervical cancer.
DES was prescribed to pregnant women between 1940 and 1971 to prevent miscarriage. A small number of women whose mothers were given this drug have developed a rare type of vaginal and cervical cancer called adenocarcinoma. Fortunately, the incidence of DES-related cancers is decreasing. This is because most of the DES-related cancers have arisen in women younger than 25 years of age, and virtually all before the age of 30 years.
Women who think they have been exposed to DES should inform their clinician and have a special type of Pap test performed yearly. Further information can be obtained from DES Action USA (www.desaction.org) and DES Cancer Network (www.descancer.org).
Other behaviors, such as diet, may play a role in cervical cancer.
Those whose diets are lacking in fruits and vegetables may be more likely to get many types of cancer.
The risk for cervical cancer increases with age.
Because full-blown cervical cancer typically takes years to develop, women between the ages of 35 and 50 are the ones who are most frequently diagnosed with the disease. However, women older than 50 and postmenopausal women are not protected from cervical cancer. 25% of cervical cancer cases and 41% of deaths occur in women aged 65 and older.
At one point, researchers thought that celibate women such as nuns did not develop cervical cancer, but this is no longer considered true. Therefore, it is important for all women to get routine Pap smears throughout adulthood.
Diagnosis
A Pap test can detect cervical changes at a very early
Your clinician or gynecologist can do a Pap test during a regular pelvic examination. He or she will use a plastic or metal instrument (speculum) to open your vagina and take a sample of your cervical cells with a small brush, swab, or scraper. The cells will be spread onto a glass slide and sent to a lab where they will be examined under a microscope and analyzed.
An abnormal result does not mean you have cancer, or even precancer. It is possible that you had an infection at the time the sample was collected, or that too few cells were taken. In the case of an abnormal Pap test result, your clinician may wish to repeat the test or perform more tests.
If abnormalities are detected on a Pap test, colposcopy may be recommended. Colposcopy allows your clinician to take a close look at your cervix.
A colposcope is a viewing instrument with a magnifying glass that enables your clinician to see problems that are not visible to the naked eye. As with a Pap test, you will have a speculum inserted to open your vagina so that the colposcopy can be performed. During the test, your cervix will be bathed with a solution that makes the cells easier to see. This may cause mild burning.
If there is evidence of abnormal tissue development (dysplasia such as cervical intraepithelial neoplasia) or another abnormality, your clinician may take a sample of the affected tissue for analysis (biopsy).
A biopsy can identify what type of cervical problem you have.
A biopsy is a procedure in which a small piece of tissue is removed and examined under a microscope. Biopsy samples of the cervix can be collected during a colposcopy. The clinician can also obtain samples by scraping the cervix (endocervical curettage). Larger biopsies are usually performed using other procedures, such as a loop electrosurgical excision procedure (LEEP), in which abnormal tissue is cut out. Any biopsy method may cause mild cramping, pain, or bleeding afterward.
If invasive cervical cancer is found, your clinician will order more tests to determine how far it has progressed. Establishing the stage of your cancer is essential for determining an appropriate course of treatment.
Treatment of cervical cancer is guided by the stage of the cancer. The stages of cervical cancer range from I to IV; stage I is the earliest and most treatable. Stage IV cancer – cancer that has spread (metastasized) beyond the pelvis to other parts of the body – is the most advanced form and the hardest to cure.
To stage your cancer, your clinician will take your medical history and perform a thorough examination of your cervix and pelvic region. A larger tissue sample may be taken to see how far the cancer has penetrated your cervix. A rectal exam and sigmoidoscopy (examination of the lower part of the colon with a flexible scope) may be performed to rule out cancer in your rectum and bowel. A cystoscope can be used to check the inside of your bladder for signs of cancer. Your blood will be analyzed and your liver and kidney functions checked. Your clinician may order a CT scan of your pelvic and abdominal region to check for evidence of cancer spread (metastasis).
Prevention and Screening
Waiting to have sex and limiting the number of your sexual partners are the best ways to reduce your chances of getting human papillomavirus (HPV), a major risk factor of cervical cancer.
Using a condom during sex can help reduce your chances of contracting HIV, but condoms may not protect against HPV. Both of these sexually transmitted infections predispose women to cervical cancer.
Not smoking or quitting if you do smoke can lower your risk of getting cervical cancer.
Routine Pap tests can detect cervical problems early, when cancer can be prevented or cured.
Since the Pap test was introduced, the death rate from cervical cancer has been cut in half. If all women underwent regular Pap screening, death from this cancer could almost be eliminated. This is because the Pap test can detect changes in the cells of the cervix (cervical intraepithelial neoplasia, or CIN) at a very early stage, before symptoms are apparent, allowing for prompt diagnosis and successful treatment.
The American Cancer Society recommends that all women have a yearly Pap test starting at age 18 or at the age they become sexually active. Some clinicians think that if the results are normal for 3 years in a row, Pap tests need to be performed only every 2 to 3 years. Older women should continue to have Pap tests because a large percentage of deaths from cervical cancer occur in women aged 65 and older.
Urgent Care
If you experience abnormal vaginal bleeding or discharge, see your clinician.
Treatment Options
Drug Therapy
Your doctor is the best source of information on the drug treatment choices available to you.
Other Therapies
Often, mild abnormal changes in the cells on the surface of the cervix (dysplasia) do not require treatment and may disappear over a period of careful watchful & waiting.
If you do not wish to or cannot undergo surgery, or if your cancer is more advanced, your clinician may recommend radiation therapy.
Radiation therapy uses high-energy rays to kill cancer cells and shrink tumors. Radiation can be delivered from an outside source or from radiation-producing materials placed directly in or around a tumor.
The side effects of radiation may include fatigue, skin changes, loss of appetite, nausea, and diarrhea. These side effects are usually temporary. Sometimes, radiation in the pelvic region results in scar tissue that narrows the vagina, which could make sex uncomfortable or painful. Early menopause and urination problems can occur as well.
If cancer has penetrated deeply into your cervix or beyond, your clinician may recommend chemotherapy as part of your treatment regimen.
Chemotherapy is given to women with bulky tumors in the cervix or in the cervix and upper part of the vagina. The combination of chemotherapy and radiation therapy is more effective than radiation alone. The same holds true for women whose cancer has spread throughout the pelvic area or to organs close to the cervix such as the bladder and rectum.
The chemotherapy that is given along with radiation is called low-dose chemotherapy and is used to make radiation therapy more effective. Because the doses are low and the rate of administration is slow, the side effects are minimal and considerably less severe than one would expect with conventional (full-dose) chemotherapy.
Full-dose chemotherapy is given to patients with cancer that has spread beyond the pelvis to other areas of the body, such as the lungs or lymph nodes in the neck.
Chemotherapy drugs (typically given by mouth or through a vein) kill cancer cells, but they kill healthy cells as well. Full-dose chemotherapy can lead to side effects such as hair loss, nausea, vomiting, and diarrhea. The effects are temporary and generally resolve once chemotherapy is stopped.
During full-dose chemotherapy, some of the unpleasant side effects can be minimized with other medications. Chemotherapy also weakens the immune system. People undergoing chemotherapy are more vulnerable to infection. The likelihood of bleeding and bruising after minor injuries is also increased during chemotherapy.
Surgery
Most mild dysplasias do not require treatment and often disappear over a period of careful watchful waiting. Those that persist may require surgical treatment.
If you have more severe dysplasia, a variety of minor surgical procedures can be used to remove it.
Dysplasias and carcinoma in situ (certain types of cervical intraepithelial neoplasia, or CIN) can be treated on an outpatient basis using any one of a number of techniques. These treatments generally require only local anesthesia. Abnormal cervical tissue can be destroyed via freezing (cryotherapy), light (laser surgery), or heat (electrosurgery).
Most severe CIN lesions are treated with a loop electrosurgical excision procedure (LEEP), a highly effective minor operation. During a LEEP, abnormal tissue is cut out with a thin wire loop that has an electrical current passing through it. This can be performed in a clinician’s office with local anesthesia in most cases. Another way to remove large pieces of tissue is conization, in which a wedge-shaped piece of the cervix is taken out. A conization can also be performed using a LEEP.
Treatment of invasive cervical cancer consists of surgery, radiation, and chemotherapy. Your treatment options depend on your age, overall health, whether you want to have children, and the stage of your cancer.
If you are young and healthy and are in the earliest stages of the disease, one option would be to have the cancer removed surgically. If you do not plan to have children, you might opt to have your uterus removed (hysterectomy).
Treatment Options for Invasive Cervical Cancer By Stage
Stage 1
- Conization
- Hysterectomy with or without lymph node removal
- Hysterectomy plus lymph node removal with or without radiation
- Radiation with or without chemotherapy
Stage 2
- Radiation with or without chemotherapy
- Hysterectomy plus lymph node removal with or without radiation and chemotherapy
Stage 3
- Radiation and chemotherapy
Stage 4
- Radiation
- Chemotherapy
- Radiation and chemotherapy
If your cancer is more advanced or if you are an older woman in poor health, radiation might be your primary treatment choice. If your cancer has spread, adding chemotherapy to surgery and/or radiation therapy might be recommended.
If you do not wish to have children or if you have more extensive cervical cancer, removal of the entire uterus and cervix (hysterectomy) is an option.
If you decide to have a hysterectomy, your entire uterus and cervix will be removed; not just the cancerous parts. The uterus may be removed through the vagina (vaginal hysterectomy) or through an incision in the abdomen (abdominal hysterectomy), depending on your circumstances. In some cases, the ovaries and fallopian tubes are taken out as well.
In most cases of extensive cervical cancer, a modified radical or radical abdominal hysterectomy is performed. With a radical hysterectomy, all of your cervix, part of your vagina, your uterus, and nearby lymph nodes are removed.
Special Circumstances
If you are pregnant and develop cervical cancer, your options depend on the stage of your cancer.
If your cancer is in its early stages, it may be safe to wait until after you have given birth to undergo treatment. If your cancer is in a later stage, you and your clinician need to discuss whether you should continue the pregnancy. If you decide to carry it to term, the baby will be delivered via cesarean section as soon as it can survive outside the womb. If you have very advanced cancer, immediate treatment is your safest choice.
Prognosis
Your long-term outlook depends on which stage your cancer was in when it was discovered and how well you responded to your treatments.
If your cancer was caught early, your chance of a cure is high. In general, nearly every case of early cervical cancer can be treated and cured. The cure rate drops sharply when the cancer is advanced and has spread to distant parts of the body.
Follow-Up
Because cancer can come back, you will need to see your clinician regularly.
Your clinician may wish to see you as frequently as every 3 months for exams and Pap test during the first year after your cancer diagnosis. If everything looks good, your clinician may decrease the frequency of exams and tests to every 6 months.
If you are experiencing signs or symptoms of this issue, or have questions, you can schedule an appointment with us at our Baldwin Park office in Orlando, FL.
Source: PDR.net