Many women have pain in their pelvic region at some point in their lives. Finding the cause of pelvic pain can be a long process. Often there is more than one reason for the pain and its exact source can be hard to detect. Women who have pelvic pain should consult a doctor, especially if the pain disrupts daily life or gets worse over time. This page explains:
- Some causes of pelvic pain
- How it is diagnosed
- How it is treated
Because pelvic pain has a number of causes, finding the source can be a long and complex process. Even when there is no specific cause found, there are treatments that can help.
Types of Pelvic Pain
Pelvic pain can vary in how it is felt and when it occurs. It can come and go for brief times or it can be constant. Sometimes pelvic pain can recur on a regular cycle or schedule. It also may occur only at certain times—before or after eating, while you urinate, during sex, or during a menstrual period.
Some women may feel pain almost every day. This may mean that a problem has gotten worse. Over time, it may become more difficult to cope with the pain. When this occurs, a woman may feel pain at some times more than others, even though the problem has not gotten worse.
Pelvic pain can disrupt a woman’s work, movement, sexual relations, sleep, or family duties. Not knowing the cause of the pain can make it even more stressful. When pain has been present for a long time, it can affect a woman’s mental and physical health. Pelvic pain that lasts for more than 6 months and does not improve with treatment is called chronic pelvic pain. The type and nature of pelvic pain—whether it comes and goes or is constant, is sharp or dull, is in one place or a broad area—will help your doctor detect the cause of the problem.
Causes
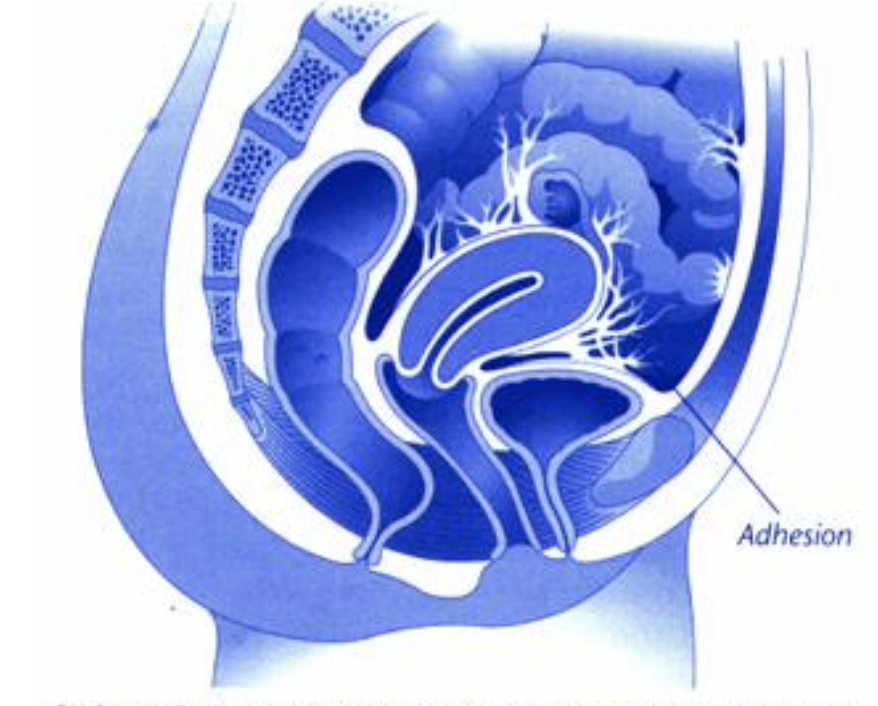
Pelvic pain often is caused by a variety of factors. It can be acute or chronic, depending on the cause. Acute (sharp) pain starts over a short time (a few minutes to a few days). Chronic pain can either come and go or be constant. Pelvic pain can result where scar tissue (adhesion) forms. In evaluating the cause of pelvic pain, your doctor may ask you questions about the pain and its effect on your daily life.
All causes of pain should prompt a visit to your doctor. Your medical history will be taken and you will have a physical exam. Some tests also may be done to find the cause. Your doctor may then be able to suggest treatment.
Acute Pelvic Pain
Acute pelvic pain often has a single cause. This type of pain may be a warning that something is wrong, such as an infection, ovarian cysts, or an ectopic pregnancy.
Infection
An infection or inflammation of a woman’s reproductive organs can cause pelvic pain. But, the infection does not have to be in the reproductive organs to cause pelvic pain. The source may be the urinary tract, bowel, or even the appendix.
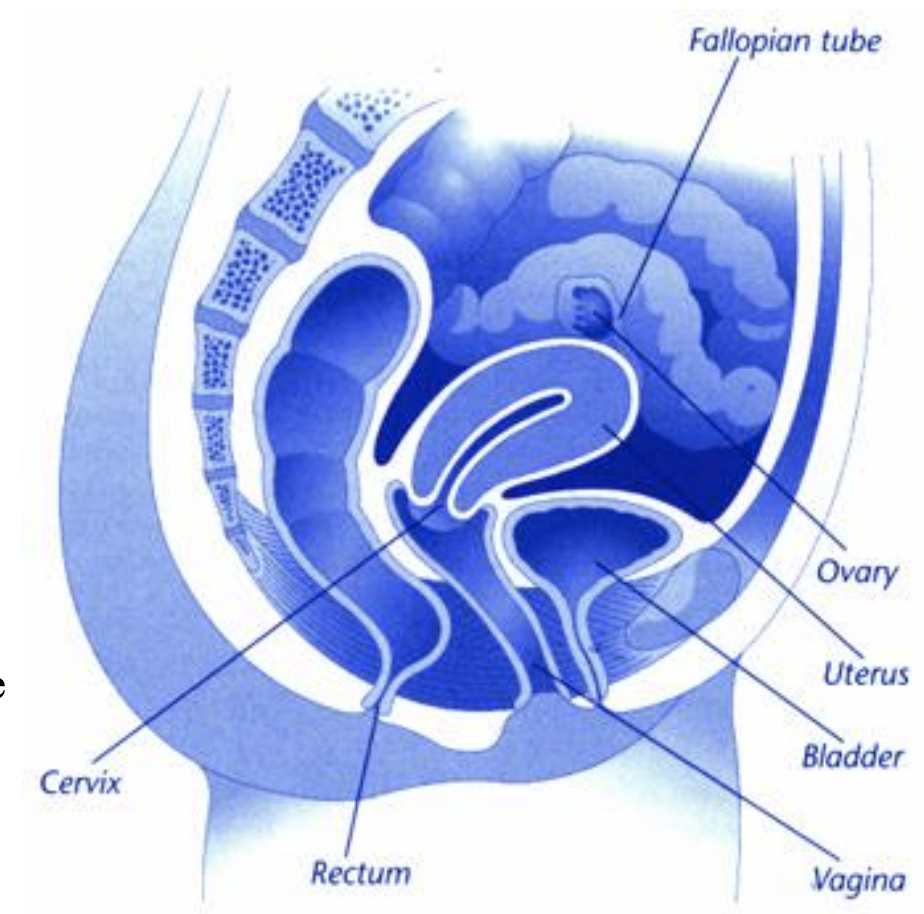
Pelvic inflammatory disease (PID) is a term used to describe infection of the uterus, fallopian tubes, and ovaries. Symptoms of PID include fever and pain in the lower pelvic area. The pain often is a mild ache, but it can be severe.
Infections of the urethra, bladder, or kidneys (urinary tract infections) may cause pain. These conditions can cause pain while urinating, and you may have a strong and frequent urge to urinate even when little urine is there. If back pain occurs, the infection may have spread to the kidneys. Your doctor may prescribe antibiotics to treat this pain.
In most cases, a vaginal infection (vaginitis) does not cause pelvic pain. However, in some cases, it can be painful, mainly during and after sex. Many kinds of organisms can cause vaginal infections, and most can easily be treated.
Ovarian Cysts
A cyst is a sac filled with fluid. Some cysts on the ovaries form as a result of the normal process of ovulation that occurs each month in a woman’s menstrual cycle. Often a cyst goes away on its own within a day or two. Some cysts can persist. These cysts often are felt as a dull ache or heaviness. Sometimes they cause pain during sex. Sharp pain can occur if a cyst leaks fluid or bleeds a little. This may happen around the middle of the menstrual cycle.
A cyst often can be detected by a pelvic exam. In some cases, ultrasound (a test in which sound waves are used to view organs) is needed. Rarely, severe, sharp, and constant pain results when a large cyst twists. Large cysts and those that do not go away on their own within a few months may need to be removed by surgery.
Ectopic Pregnancy
An ectopic pregnancy is one that grows outside the uterus, often in a fallopian tube. This is more likely to occur in women who have some damage to their tubes. With an ectopic pregnancy, the pain often starts on one side of the abdomen after a missed period. Vaginal bleeding or spotting may occur with the pain. This problem needs urgent care and may require surgery. An ectopic pregnancy can lead to bursting of the fallopian tube and bleeding inside the abdomen. This condition can be life threatening.
Chronic Pain
Chronic pain that comes and goes often has a distinct cause. Constant chronic pain may be caused by more than one problem. Often a woman has more than one cause of pain that involves several systems of the body. Some conditions start with pain that comes and goes and then becomes constant. In some women, the pain occurs in cycles.
Dysmenorrhea
Although some mild pain is common during a woman’s menstrual period, some women have severe pain, which is called dysmenorrhea. It may be caused by prostaglandins, which are made by the lining of the uterus. This may cause spasms or cramping of the uterus.
Ovulation Pain
Pain that is felt around the time of ovulation is sometimes called mittelschmerz (German for “middle pain”). Ovulation occurs in the middle part of the menstrual cycle. This pain can range from a mild pinch or twinge to something more severe. In some women it occurs every month.
Endometriosis and Adenomyosis
If menstrual cramps get worse over time or remain strong beyond the first 1 or 2 days of menstrual flow, they may be caused by endometriosis or adenomyosis.
Endometriosis is a condition in which tissue similar to that normally lining the uterus is found outside of the uterus, most often on the ovaries, fallopian tubes, and other pelvic structures. The cause of endometriosis and the reasons for pain during the menstrual cycle are not known for sure. Endometriosis often makes menstrual cramps more severe. It also can cause pain at other times of the month or during sex.
Adenomyosis occurs when the lining of the uterus extends into the muscle wall of the uterus. The cause of this often is unknown. This condition can cause menstrual cramps. It also can cause pressure and bloating in the lower abdomen before menstrual periods and more bleeding during periods.
Fibroids
Fibroids are benign (not cancer) growths that occur on the inside of the uterus, on its outer surface, or within the wall of the uterus. The cause of fibroids is not known. Estrogen may play a role in their growth.
Fibroids often cause no symptoms. When symptoms do occur, they may include heavier or more frequent menstrual periods and pain or pressure in the abdomen or lower back. Fibroids attached on a stem may become twisted and cause more acute symptoms.
Other Causes
In some cases, pelvic pain is not related to the reproductive organs. Other causes of lower abdominal and pelvic pain include:
- Gastrointestinal problems, including diverticulitis (inflammation of a pouch bulging from the wall of the colon), irritable bowel syndrome (a condition that may cause bouts of diarrhea and constipation and often seems to be related to stress), inflammatory bowel disease, constipation, or cancer.
- Urologic problems, including stones, infection, incontinence, cancer of the bladder, and interstitial cystitis (inflammation of the bladder wall and lining).
- Muscular and skeletal problems, including lower back pain, herniated disks, pelvic floor muscle spasms, and fibromyalgia (a condition that causes pain and tenderness in certain tissues and muscles).
- Psychologic disorders, including depression.
Diagnosis
Because there are so many causes of pelvic pain, your doctor will need to know more about your pain. Although this process may seem complex and time consuming, it is the best way to find out what is causing the pain.
History
Your doctor will ask about the degree and location of the pain. He or she also will ask about when it started, when and how often you feel it, and how it affects your daily life. The doctor may ask about your medical and sexual history, any past pregnancies, and about any physical, sexual, or mental abuse.
Women who have a history of depression or sexual abuse or have been raped are more likely to have chronic pain. For these reasons, your doctor may ask many questions about you and your family to see if there is a need for counseling.
Your doctor may ask you to keep a journal in which you describe the exact nature of the pain (see box). What you write down can help your doctor rule out certain causes. Bring it with you when you see your doctor. Your doctor may consult with or refer you to others for care. The type of care depends on the nature of the problem and its possible cause.
Tests
After a pelvic exam is performed, certain lab tests may be needed. Sometimes, depending on the symptoms and the results of the lab tests, you may need imaging studies or other procedures to find the cause of pain:
Ultrasound: A test in which sound waves are reflected off the internal organs, producing an image that can be viewed on a screen
Cystoscopy: A test in which a slender metal tube with a lens and light source is used to view the inside of the bladder and the urethra
Laparoscopy: A surgical procedure in which a slender, light-transmitting instrument, the laparoscope, is used to view the pelvic organs or perform surgery
Colonoscopy: An exam of the entire colon using a small, lighted instrument
Pain Journal
A record of your pain will help your doctor find its cause. You may be asked to keep a pain journal so that more complete information can be obtained. In your pain journal, note when you feel pain:
- Time of day
- At certain times of your menstrual cycle
- Before, during, or after:
- Eating
- Urination
- Bowel movement
- Sex
- Physical activity
- Sleep
Describe the pain and note how long it lasts:
- Is it a sharp stab or a dull ache?
- Does it come in waves or is it steady?
- How long does it last?
- How intense is it?
- Does it always occur in the same place(s)?
- Is it mostly in one place or over a broad area?
- What makes it better or worse?
- Sigmoidoscopy: A test in which a slender device is placed into the rectum and lower colon to look for cancer
- Computed tomography (CT): A type of X-ray that shows internal organs and structures
- Magnetic resonance imaging (MRI): A method of viewing internal organs and structures by using a strong magnetic field
- Intravenous pyelography (IVP): A type of X-ray taken after fluid is injected into a vein and excreted by the kidneys
- Barium enema: A solution given through the rectum that helps problems in the colon to show up on X-rays
Treatment
If the cause of the pain is known, it is treated. If it is not known, your doctor may suggest ways to lessen or relieve the pain or to avoid making it worse.
Medications
Infections are treated with medication. If you have had a problem such as a urinary tract infection or vaginitis and it has come back, your doctor may prescribe an antibiotic. Most symptoms will improve within 1 or 2 days.
Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, can help to lessen the pain of dysmenorrhea. If they do not work, prescription drugs may help.
Some conditions can be treated with hormones. Birth control pills can be used to relieve dysmenorrhea. Other hormones can shrink some types of growths, such as endometriosis and fibroids. But, when treatment is stopped, symptoms may return.
Antidepressants have been used in some patients who have pelvic pain. They may be used alone or with other treatments.
When treating chronic pain, it is better to use a pain medication on a routine basis. Most people try to use as little pain medication as they can. But, it is not a good idea to wait until the pain is severe before you take it. Pain medication may only take the edge off the pain once the pain becomes too severe. It may not get rid of it.
Surgery
Certain problems may be treated with surgery. It can range from minor procedures to major surgery. The type of surgery depends on the exact problem. It can be done on an outpatient basis, such as laparoscopy, or it may require a stay in the hospital. Your doctor will discuss your options with you, including the risks and benefits, based on your exact problem.
Other Treatments
Heat therapy, muscle relaxants, nerve blocks, mental exercises, and physical therapy all may help treat pelvic pain. Physical therapy includes exercise, stretching, and massage. This type of treatment helps increase muscle strength and relax strain or tension. Good posture and regular exercise also can help reduce pain.
Other treatments include:
- Trigger point injections: a shot of medication into the spot that is painful
- Nutrition therapy: use of vitamin B1 and magnesium to relieve dysmenorrhea
- Acupuncture: one of several ways to stimulate nerves to reduce pain
Some types of therapy teach you mental techniques to help cope with pain. It can include relaxation exercises. These practices help change your emotional response to the pain. Biofeedback is a method used for self-control of pain.
Sometimes the doctor may suggest that you get counseling. Learning techniques that help you relax or manage stress may help ease the pain.
Finally. . .
Because pelvic pain has a number of causes, finding the source can be a long and complex process. Even when there is no specific cause found for pelvic pain, there are treatments that may help. Working with your doctor and other members of your health care team can help find the treatment that works best for you.
Glossary
Adhesion: Scarring that binds together the surfaces of tissues.
Antidepressants: Medications used to treat depression.
Biofeedback: A technique in which an attempt is made to control body functions—such as heartbeat or blood pressure.
Dysmenorrhea: Discomfort and pain during the menstrual period.
Ectopic Pregnancy: A pregnancy in which the fertilized egg begins to grow in a place other than inside the uterus, usually in the fallopian tubes.
Estrogen: A female hormone produced in the ovaries during the entire menstrual cycle.
Incontinence: Inability to control bodily functions such as urination.
Pelvic Exam: A manual examination of a woman’s reproductive organs.
Pelvic Inflammatory Disease: An infection of the uterus, fallopian tubes, and nearby pelvic structures.
Prostaglandins: Chemicals that are made by the body that have many effects, including causing the muscle of the uterus to contract, usually causing cramps.
Source: acog.org