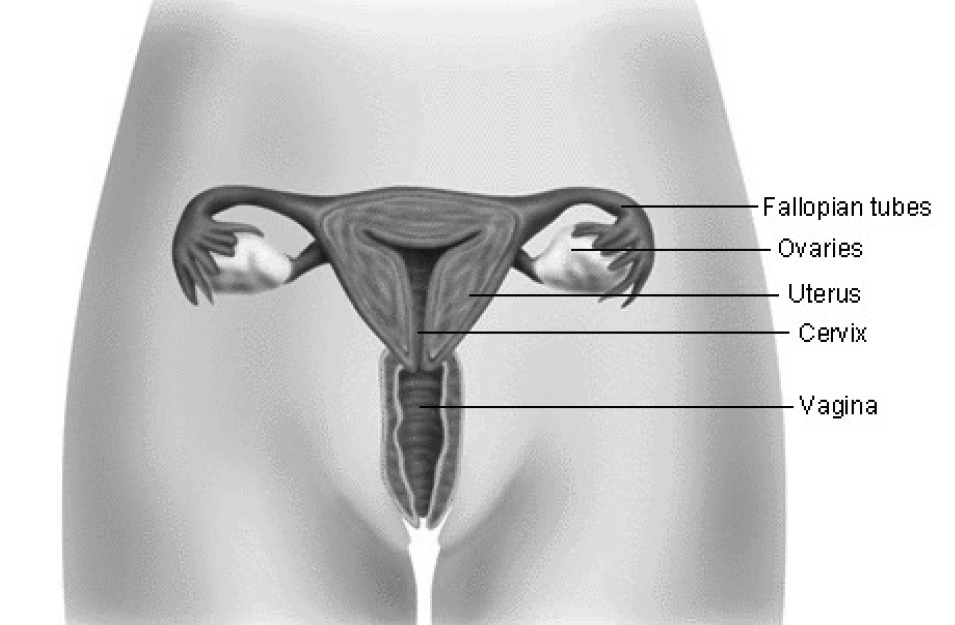
The uterus is made up of three parts: the muscle wall, the endometrium (lining), and the cervix (opening). Cancer of the uterus affects the muscle and endometrium, and in some cases, the cervix. It is good to know the risk factors and the warning signs. If the cancer is found and treated early, as many as 9 out of every 10 women who have it can be cured.
This page will explain:
- Risk factors for uterine cancer
- Symptoms
- How it is treated
If you have endometrial cancer, talk to your doctor. In most cases, this type of cancer is very treatable.
What is Cancer?
Normally, healthy cells that make up the body’s tissues grow, divide, and replace themselves on a regular basis. This keeps the body healthy. Sometimes certain cells develop abnormally and begin to grow out of control. When this occurs, growths or tumors begin to form. Tumors can be benign (not cancer) or malignant (cancer). Malignant tumors can invade and destroy nearby healthy tissues and organs. Cancer cells also can spread (or metastasize) to other parts of the body and form new tumors.
The most common type of cancer of the uterus is called endometrial cancer (adenocarcinoma). This can occur when cancer forms from the lining of the uterus. Sarcomas are another type of uterine cancer. They arise from muscle and other tissue. Although rare, this type of uterine cancer is more aggressive than adenocarcinoma and has different symptoms. Because endometrial cancer is more common and its symptoms differ from those of sarcoma, this page will focus on endometrial cancer.
Who is at Risk for Endometrial Cancer?
Endometrial cancer is the most common gynecologic cancer in the United States. About 2 or 3 women out of every 100 women will develop endometrial cancer during their lifetime.
Endometrial cancer is rare in women younger than 40 years. It most often occurs in women around age 60 years. Some women have a higher risk than others (see box). Some risk factors may be related to the use of estrogen. Estrogen is a hormone produced in a woman’s ovaries. It can be taken after menopause, when a woman’s ovaries stop producing estrogen (hormone therapy). Taken alone, estrogen increases the risk of endometrial cancer, if a woman still has her uterus. When estrogen is taken with another hormone, progesterone, a woman is protected against this increase.
Risk Factors
Certain factors can increase a woman’s risk of uterine cancer such as:
- Obesity
- Irregular menstrual periods
- Never having a baby
- Infertility
- Starting menstrual periods at an early age (before age 12 years)
- Late menopause
- History of cancer of the ovary or colon
- Use of tamoxifen to treat or prevent breast cancer
Family history of endometrial cancer- History of diabetes, hypertension, gallbladder disease, or thyroid disease
- Long-term use of estrogen without progesterone to treat menopause
- Long-term use of high-dose birth control pills
- Cigarette smoking
Symptoms
The key to finding endometrial cancer early is being alert to its symptoms. Abnormal bleeding, spotting, new discharge from your vagina, or bleeding or spotting after menopause all are symptoms of endometrial cancer. These symptoms may be constant or come and go. The cause of any abnormal bleeding or discharge, especially after menopause, should be checked by your doctor.
Diagnosis
There are no screening tests to detect endometrial cancer in women with no symptoms. But most women who have endometrial cancer have early symptoms. Several methods may be used to detect whether endometrial cancer is present:
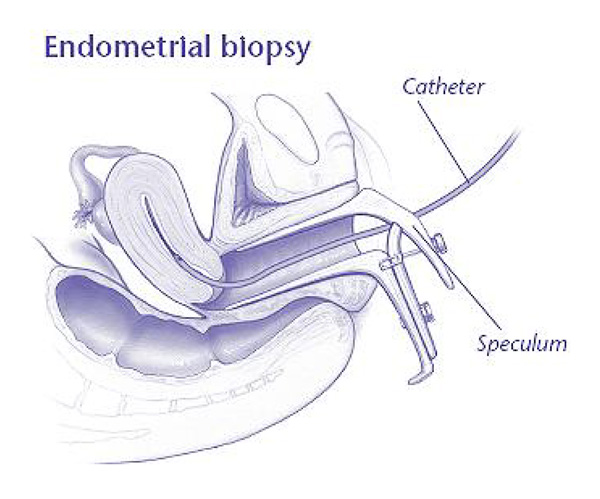
- Endometrial biopsy: A test in which a small amount of the tissue lining the uterus is removed and examined under a microscope. This will likely be the first step in checking for abnormal cells.
- Vaginal ultrasound: A test in which sound waves are used to check the thickness of the lining of the uterus and the size of the uterus.
- Hysteroscopy: A surgical procedure in which a slender, light-transmitting scope is used to view the inside of the uterus or perform surgery.
- Dilation and curettage (D&C): A procedure in which the cervix is opened and tissue is gently scraped or suctioned from the inside of the uterus.
For many women, a Pap test may be part of a regular checkup, but it may not always detect endometrial cancer. In fact, most women with endometrial cancer have normal Pap test results. Endometrial cancer can be diagnosed only by examining tissue from the uterus.
Treatment
The type of treatment you receive depends on your health and your condition. Talk to your doctor about what option is best for you.
Surgery
If endometrial cancer is found, surgery usually is done to treat the disease and find out if further treatment is needed. During surgery, the stage of disease is determined. Staging helps your doctor decide what treatment has the best chance for success. Stages of cancer range from I to IV. Stage IV is the most advanced. The stage of cancer affects the treatment and outcome.
Most patients have both hysterectomy and salpingo-oophorectomy. In most cases, this is done through the abdomen. Rarely, it can be done through the vagina. It also can be done with laparoscopy. Even though the cancer is in the uterus, the ovaries may be removed because women with uterine cancer have an increased risk of ovarian cancer. Lymph nodes in the pelvic region also may be removed and tested to find out if the cancer has spread.
Radiation
Radiation therapy may be done after surgery based on the stage of the disease. Although rare, some women are treated with radiation alone. Radiation stops cancer cells from growing by exposing them to high-energy rays. The treatment usually lasts several weeks and can require daily visits to a special center.
Other Treatments
Other forms of treatment include chemotherapy or hormone therapy. Some women may be treated with progestin, a synthetic version of the hormone progesterone. This form of treatment may be tried in the following situations:
- Surgery is not an option.
- Tests show that the cancer has spread or come back after surgery or radiation.
- A younger patient wants to have a baby in the future.
After Treatment
Women who did not receive radiation should see their doctors every 3–4 months for 2–3 years to make sure the treatment is working. After that, they should see their doctors twice a year. Women who did receive radiation may be able to see their doctors less frequently. With stage I disease, 85–90% of women will have no sign of cancer 5 or more years after treatment. The chance of a cure decreases with more advanced disease (higher stage).
Finally
If you have endometrial cancer, talk to your doctor. In most cases, this type of cancer is very treatable. Your doctor and the other people involved in your care may be able to help you get well and keep you healthy.
Glossary
Adenocarcinoma: Cancer arising in glandular tissue, such as the uterus.
Hormone Therapy: Treatment in which estrogen, and often progestin, is taken to help ease some of the symptoms caused by low levels of these hormones.
Hysterectomy: Removal of the uterus.
Laparoscopy: A surgical procedure in which a slender, light-transmitting instrument, the laparoscope, is used to view the pelvic organs or perform surgery.
Lymph Nodes: Collections of tissue that filter the flow of lymph (a nearly colorless fluid that bathes body cells) through the body.
Menopause: The process in a woman’s life when ovaries stop functioning and menstruation stops.
Pap Test: A test in which cells are taken from the cervix and vagina and examined under a microscope.
Salpingo-oophorectomy: Removal of the ovary and fallopian tube.
Stage: Stage can refer to the size of a tumor and the extent (if any) to which the disease has spread.
Tumor: Growth or lump made up of cells.
Source: acog.org